
Revista Científica UDO Agrícola
Volumen 9. Número 3. Año 2009. Páginas: 700-704
Comparison of the antibacterial activities of
different brands of Ciprofloxacin
Comparación de la actividad antibacterial de diferentes
marcas de Ciprofloxacina
Muhammad Shahid NAZIR MUGHAL![]() , Muhammad Tahir
ASGHAR, Muhammad Atif ZIA and Tariq ISMAIL
, Muhammad Tahir
ASGHAR, Muhammad Atif ZIA and Tariq ISMAIL
Pharmaceutical Lab, Punjab Institute
of Paramedical Studies. 13 Mamdot Block Mustafa Town Lahore Pakistan. E-mail:
shahidbiochemist@yahoo.com ![]() Corresponding author
Corresponding author
|
Received: 02/23/2009 |
First
reviewing ending:
05/12/2009 |
|
First
review received:
09/01/2009 |
Accepted: 09/02/2009 |
ABSTRACT
The present study
was carried out to evaluate and compare the antibacterial susceptibility of
Gram-positive and Gram-negative bacteria to Cyrocin (Ciprofloxacin). The
following three bacterial strains were used: Staphyloccocus aureus [ATCC 25923], Escherichia coli [ATCC 25922] and Pseudomonas aeruginosae [ATCC 27853]. Standard commercial discs of
definite potency are used as reference standard (Ciprofloxacin 5mg [CTO425B - OXOID Ltd. UK]).
The
test products were 250 mg and 500 mg tablets of the following brands: Cyrocin
(Highnoon Laboratories Limited), Ciproxin (Bayer Pharma (Pvt) Ltd. – Pakistan),
Mercip (Merck Marker (Pvt.) Ltd., Pakistan) and Axcin (Sandoz - Norvatis Pharma
Ltd., Pakistan). The media used were: Nutrient Broth (Cat. No. 1.05443, Merck,
Germany) and Mueller Hinton Agar [Oxoid]. The study showed no statistically
significant difference in the results of different brands.
Kew words: Antibacterial
properties, Staphyloccocus aureus, Escherichia coli, Pseudomonas aeruginosae, Ciprofloxacin
RESUMEN
El presente estudio se realizó para evaluar y comparar
la susceptibilidad antibacterial de las bacterias Gram-positiva y Gram-negativa
al Cyrocin (Ciprofloxacina). Se usaron las cepas bacetriales Staphyloccocus aureus [ATCC 25923], Escherichia coli [ATCC 25922] y Pseudomonas aeruginosae [ATCC 27853]. Se
utilizaron discos comerciales estandars de potencia definida como estandar de
referencia (Ciprofloxacin 5mg [CTO425B - OXOID Ltd. UK]). Los productos evaluadoes fueron tabletas
de 250 mg y 500 mg de las siguientes marcas: Cyrocin (Highnoon Laboratories
Limited), Ciproxin (Bayer Pharma (Pvt) Ltd. – Pakistan), Mercip (Merck Marker
(Pvt.) Ltd., Pakistan) y Axcin (Sandoz - Norvatis Pharma Ltd., Pakistan). Los
medios usados fueron: Nutrient Broth
(Cat. No. 1.05443, Merck, Germany) and Mueller Hinton Agar [Oxoid]. El estudio
mostró diferencias estadísticamente no significativas en los resultados de las
diferentes marcas,
Palabras clave: Propiedades antibacteriales, Staphyloccocus aureus, Escherichia
coli, Pseudomonas aeruginosae,
Ciprofloxacina
INTRODUCTION
Antimicrobial
susceptibility tests measure the ability of an antibiotic or other
antimicrobial agents under suitable conditions to inhibit bacterial growth in vitro (Inhibitory effect on
micro-organism) (Bauer et al. 1966).
For
evaluating the safety and effectiveness of antibiotic products, several types
of antimicrobial susceptibility (sensitivity) tests are recommended. The choice
of the method depends on local needs and resources, however, the disk diffusion
test has a long and successful track record; it is still the most common test
used for antimicrobial susceptibility testing. In this method, the paper discs
impregnated with a defined quantity of antimicrobial agent are placed on agar
medium uniformly seeded with test organism. A concentration gradient of the
antibiotic forms by diffusion from the disc and growth of test organism is
inhibited at a distance from the disc that is related among other factors to
the susceptibility of the organism.
The
modified “Kirby Bauer Method” is the recommended method by National Committee
on Clinical Laboratory Services (NCCLS-USA) subcommittee on Antimicrobial
Susceptibility testing (Bauer et al. 1966).
The Bauer Kirby procedure has been standardized to correlate the zone diameter
produced by the fixed amount of antimicrobial agent in the disc with an MIC for
the drug–organism combination. The results may be interpreted as resistant,
intermediate, moderately susceptible or susceptible. The term intermediate is
important. It generally means that the result is inconclusive for that
drug-organism combination. The term moderately susceptible is applied to those
situations where a drug may be used for infections in a particular body site,
e.g. cystitis, because it is highly concentrated in the urine. The interpretive
standards for Ciprofloxacin 5 µg disc are given by National committee for
clinical laboratory standards is: Resitatant £ 15; Intermediate
16-20 y Susceptible ³ 21.
Ciprofloxacin (Cipro®) was discovered in
1960s by Bayer. Its discovery stemmed from researchers in the 1960s looking for
an alternative treatment to malaria. Cipro® was approved in 1987 by the U.S.
Food and Drug Administration as a broad-spectrum antibiotic that is active against both
Gram-positive and Gram-negative bacteria. Since then it has been
prescribed to over 500 million patients worldwide. Cipro® has been approved for
the treatment of 14 types of infection including respiratory and urinary tract
infections, skin, and other gastro-intestinal infections (SIS, 1987). Cipro® is
the most widely used fluoroquinolone antibiotic in the world, which testifies
to its wide range of uses. It is also the first antibiotic to be approved
specifically for an indication associated with the intentional use of a lethal
biological weapon (Hilliard et al. 1995).
Cipro is available in three different forms: Tablets, Oral Suspension
(strawberry-flavored liquid to be taken by mouth), and I.V. (which a doctor or
nurse injects directly into the bloodstream) (Drusano et al. 1986).
Because of
its general safety, potency and broad spectrum activity, Ciprofloxacin was
initially reserved as a "last-resort" drug for use on difficult and drug-resistant infections. As with any
antibiotic, however, increasing time and usage has led to an increase in
Ciprofloxacin-resistant infections, mainly in the hospital setting. Also,
implicated in the rise of resistant bacteria is the use of lower-cost,
less potent fluoroquinolones, and the widespread addition of Ciprofloxacin and
other antibiotics to the feed of farm animals, which leads to greater and more
rapid weight gain, for reasons which are not clear (Brouwers, 1992). The
toxicity of drugs that are metabolised by the cytochrome P450 system is
enhanced by concomitant use of some quinolones (Janknegt, 1990). They may also
interact with the GABA A receptor and cause neurological symptoms; this is
further augmented by certain non-steroidal anti-inflammatory drugs (Krishek and
Smart, 2001).
The present study was carried out to evaluate and compare the
antibacterial susceptibility of Gram-positive (Staphylococcus aureus)
and Gram-negative (Escherichia-coli and Pseudomonas aeruginosae)
bacterial strains to Cyrocin (Ciprofloxacins) 250 mg and 500 mg tablets of
Highnoon Laboratories and three other leading brands of the same drug.
MATERIAL AND METHODS
Test organisms
The
following three bacterial strains were used for the study:
Staphyloccocus aureus [ATCC 25923]
Escherichia coli [ATCC 25922]
Pseudomonas aeruginosae [ATCC 27853]
Reference standard
Standard
commercial discs of definite potency are used as reference standard
(Ciprofloxacin 5mg [CTO425B - OXOID Ltd. UK])
Test products
The
250 mg and 500 mg tablets of the following brands were tested: Cyrocin (Highnoon
Laboratories Limited), Ciproxin (Bayer Pharma (Pvt) Ltd. – Pakistan), Mercip
Merck Marker (Pvt.) Ltd., Pakistan) and Axcin (Sandoz - Norvatis Pharma Ltd., Pakistan).
Media
Nutrient
Broth (Cat. No. 1.05443, Merck, Germany) and Mueller Hinton Agar [Oxoid].
Preparation of Turbidity Standard
The
turbidity standard was prepared by pouring 0.6ml of a 1% (10 g L-1) of solution of Barium
chloride dehydrate into a100ml graduated cylinder and making up the volume to
100ml with 1% (10ml/l) sulfuric acid.
Preparation of antimicrobial susceptibility test discs
Standard discs of
Ciprofloxacin (Andrews, 2001).
Ciprofloxacin sensitivity disc (5mg) of OXOID- UK were used as a Reference Standard.
Preparation of test disc
Discs
(6mm in diameter) were punched out from 47 mm Petri Pad (Millipore Corporation,
USA) and placed in Petri dishes allowing a distance of 2-4 mm between each disc
and sterilized in a hot air oven at 160°C for 1 hour.
The
average weight of five tablets was taken and the tablets were ground and the
powder equivalent to 50 mg was taken in a 100mL volumetric flask. Added 15-20
mL distilled water into the flask and sonicated for few minutes and made up the
volume upto the mark. An aliquot of 0.01mL (10mL) was pipetted
onto a separate disc incubated at 37°C for 1 hour placed
in labeled air tight container and kept in refrigerator at 4°C until use.
Procedure for inoculation of plates and application of
plates (The Modified Kirby Bauer Method) (Barry et al. 1980).
The inoculum is prepared
and disc is applied as per following procedure:
Inoculum
Preparation
1.
To prepare the inoculum
from culture plate, touch with a loop the tops of each 3.5 colonies of similar
appearance of the organism to be tested.
2.
To make the inoculum
from a pure culture, a loopful of confluent growth is similarly suspended in
saline.
3.
Compare the tube with turbidity standard and adjust
the density of the test suspension to that of the standard by adding more
bacteria or more sterile saline. Proper adjustment to the turbidity of the inoculum is essential to ensure that the
resulting lawn growth is confluent or almost confluent.
Inoculation
of plates and application of discs
1.
The plates were inoculated by dipping a sterile swab
into the inoculum. The excess inoculum was removed by pressing and
rotating the swab firmly against the side of the tube above the level of the
liquid.
2.
The swab were streaked all over the surface of the
medium three times rotating the plates through an angle of 60° after each
application. Finally, the swab was passed around the edge of the agar surface.
The agar was left to dry for a few minutes at room temperature with the lid
closed. The antibiotic discs were placed on the inoculated plates using a
sterile forceps.
3.
The plates were placed in an incubator at 35°C within 30 minutes
of preparation in a CO2 free atmosphere.
4.
After overnight incubation, the diameter of each zone
was measured and recorded in ‘mm’.
RESULTS AND
DISCUSSION
The
study was conducted to compare the antibacterial susceptibility of Highnoon
brands of Ciprofloxacin (i.e.
Cyrocin) 250 mg and 500 mg tablets with the pure Ciprofloxacin (as standard)
and three other leading brands of Ciprofloxacin tablets of same strength.
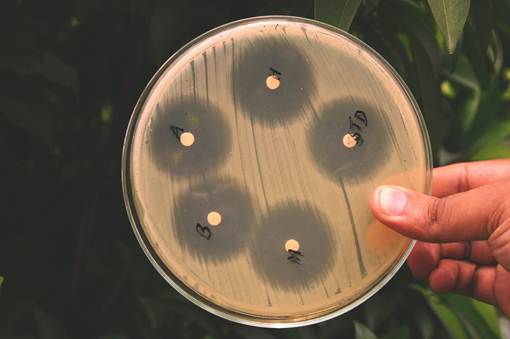
The
results of the study in terms of inhibition zone diameters produced by the 5 mg potency discs are
given in tables 1 and 2. Also, the photograph of the plates with the zone of
inhibition of different brands of Ciprofloxacin tablets against the tested
bacterial strains is given in figure 1.
|
Table
1. Antimicrobial susceptibility testing of different brands of
Ciprofloxacin 250 mg tablets |
||||||
|
Bacterial Strains |
Sample No. |
Zone of Inhibition (mm) |
||||
|
Standard |
Axcin |
Ciproxin |
Cyrocin |
Mercip |
||
|
Escherichia coli [ATCC # 25922] |
1 |
34.96 |
35.37 |
35.65 |
35.15 |
34.90 |
|
2 |
33.71 |
34.90 |
35.15 |
34.85 |
34.40 |
|
|
3 |
33.85 |
35.20 |
34.70 |
34.65 |
34.70 |
|
|
|
Avg. |
34.17 |
35.16 |
35.17 |
34.88 |
34.67 |
|
|
STDEV |
0.68 |
0.24 |
0.48 |
0.25 |
0.25 |
|
Staphylococcus Aureus [ATCC # 25923] |
1 |
24.93 |
26.15 |
26.07 |
25.80 |
25.13 |
|
2 |
24.71 |
25.50 |
25.45 |
25.30 |
24.80 |
|
|
3 |
24.80 |
24.90 |
26.10 |
25.95 |
25.30 |
|
|
|
Avg. |
24.81 |
25.52 |
25.87 |
25.68 |
25.08 |
|
|
STDEV |
0.11 |
0.63 |
0.37 |
0.34 |
0.25 |
Pseudomonas aeruginosa
[ATCC # 27853] |
1 |
27.68 |
28.69 |
29.07 |
28.28 |
28.03 |
|
2 |
27.20 |
28.10 |
28.10 |
27.70 |
27.40 |
|
|
3 |
26.90 |
27.90 |
28.65 |
27.90 |
27.75 |
|
|
|
Avg. |
27.26 |
28.23 |
28.61 |
27.96 |
27.73 |
|
|
STDEV |
0.39 |
0.41 |
0.49 |
0.29 |
0.32 |
|
Avg.: Average;
STDEV: Standard Deviation |
||||||
|
Table 2. Antimicrobial
susceptibility testing of different brands of Ciprofloxacin 500 mg tablets. |
||||||
|
Bacterial Strains |
Sample No. |
Zone of
inhibition (mm) |
||||
|
Standard |
Axcin |
Ciproxin |
Cyrocin |
Mercip |
||
|
Escherichia coli [ATCC # 25922] |
1 |
33.72 |
34.00 |
35.00 |
34.20 |
33.97 |
|
2 |
34.10 |
33.82 |
37.45 |
33.80 |
37.99 |
|
|
3 |
33.06 |
36.62 |
34.47 |
36.15 |
34.50 |
|
|
|
Avg. |
33.63 |
34.81 |
35.64 |
34.72 |
35.49 |
|
|
STDEV |
0.53 |
1.57 |
1.59 |
1.26 |
2.18 |
|
Staphylococcus
Aureus [ATCC # 25923] |
1 |
28.00 |
27.50 |
28.77 |
27.00 |
27.98 |
|
2 |
26.90 |
27.19 |
27.32 |
26.99 |
26.84 |
|
|
3 |
27.00 |
26.92 |
29.00 |
27.41 |
27.00 |
|
|
|
Avg. |
27.30 |
27.20 |
28.36 |
27.13 |
27.27 |
|
|
STDEV |
0.61 |
0.29 |
0.91 |
0.24 |
0.62 |
Pseudomonas aeruginosa
[ATCC #
27853] |
1 |
27.95 |
30.02 |
30.03 |
29.27 |
29.60 |
|
2 |
31.00 |
32.19 |
32.00 |
32.00 |
32.42 |
|
|
3 |
28.37 |
31.00 |
32.72 |
34.68 |
32.00 |
|
|
|
Avg. |
29.11 |
31.07 |
31.58 |
31.98 |
31.34 |
|
|
STDEV |
1.65 |
1.09 |
1.39 |
2.71 |
1.52 |
|
Avg.: Average;
STDEV: Standard Deviation |
||||||
|
|
|
Escherichia coli [ATCC #. 25922] |
|
Staphylococcus aureus [ATCC #. 25923] |
|
Pseudomonas aeruginosae [ATCC #. 27853] Figure 1. Zone of inhibition of different brands of Ciprofloxacin
tablets against the tested bacterial strains. |


The
comparison of the results with the NLCCS Control limits for monitoring
inhibitory zone diameters (mm) shows that all the results fall within the
acceptance range (NCCLS, 1994). The control limits for monitoring inhibitory
zone diameter with 5 mg disc content of
Ciprofloxacin for the bacterial strains is given below:
Escherichia coli (ATCC#25922): 30-40mm
Staphylococcus
aureus (ATCC#25923): 22-30mm
Pseudomonas aeruginosae (ATCC#27853): 25-33mm
The
results for 250 mg tablets were median whereas the results for 500 mg tabs fall
within the upper range.
Apparantly,
all the results are comparable and are similar than standard. Also, the results
of Ciproxin [Bayer] showed the most consistent zones of inhibition against
three studied bacterial strains followed by Mercip [Merck], Axcin [Sandoz] and
Cyrocin [Highnoon].
The
statistical analysis revealed that there is no significant difference in the
results for different brands and statistically the antibacterial activities of
all the brands are similar.
LITERATURE CITED
Andrews, J. M. 2001. BSAC standardized disc
susceptibility testing method. Journal of Antimicrobial Chemotherapy 48, Suppl.
S1: 43-57.
Barry, A. L. and C. Thornsberry. 1980.
Susceptibility Testing: Diffusion Test Procedures. In: Lennette, E. H. Manual of Clinical Microbiology. 3ª ed., ASM,
Washington D. C, U.S.A. p. 464.
Bauer, A. W.; W. M. N. Kirby, J. C. Sherris
and M. Turk. 1966. Antibiotic susceptibility testing by a standardized single
disk method. Am. J. Clin. Pathol. 45:493-496.
Brouwers, J. R. 1992. Drug interactions with
quinolone antibacterials. Drug Saf 7: 268-281.
Drusano, G. L.; H. C. Standiford, K.
Plaisance, A. Forrest, J. Leslie and J. Caldwell. 1986. Absolute oral
bioavailability of ciprofloxacin. Antimicrob Agents
Chemother 30: 444-446.
Hilliard J. J.; H. M. Krause, J. I. Bernstein,
J. A. Fernandez, V. Nguyen, K. A. Ohemeng and J. F. Barrett. 1995. A comparison
of active site binding of 4-quinolones and novel flavone gyrase inhibitors to
DNA gyrase. Adv. Exp. Med. Biol. 390: 59-69.
Janknegt R. 1990. Drug interactions with
quinolones. J. Antimicro. Chemo. 26: 7-29.
Krishek, B. J. and T. G. Smart. 2001. Proton
sensitivity of rat cerebellar granule cell GABAA receptors: dependence on
neuronal development. J. Physiol. 530 (2): 219-233.
National Committee for Clinical Laboratory
Standards (NCCLS). 1994. Performance Standards for Antimicrobial Disk and
Dilution Susceptibility Tests for Bacteria Isolated from Animals; Proposed
Standard. NCCLS document M31-P (ISBN 1-56238-258-6). NCCLS, 771 East Lancaster
Avenue, Villanova, PA 19085, USA.
Second Informational Supplement M100-S2.
(SIS). 1987. Performance standards for Antimicrobial Susceptibility Testing. 1987, National Committee for
clinical laboratory Standards, Villanova, Pa, USA.
Página diseñada por Prof. Jesús Rafael Méndez Natera
TABLA DE CONTENIDO DE LA REVISTA CIENTÍFICA UDO
AGRÍCOLA


